5 Red Flags in Your Clinical Trial Budget (And How to Fix Them)
Table of Contents
Most clinical trial budgets have problems built in from day one. The budget gets approved, the trial starts, and six months later, everyone is wondering where the money went. Here are five red flags to catch early.
Red flag #1: Unrealistic screen failure assumptions
If your budget assumes a 20% screen failure rate but your Protocol has complex inclusion/exclusion criteria, you’re in trouble. Screen failures in CNS and oncology trials routinely exceed 50%. Every screen failure costs $2,000–5,000 in site time and procedures.
Fix: Use historical data from similar studies and therapeutic areas. Add a 10–15% buffer on top of your best estimate.
Red flag #2: No budget for protocol amendments
The average Phase III trial undergoes 2–3 substantial amendments, each costing $500K+ in direct costs. If your budget doesn’t include a line item for amendments, you’re planning to fail.
Fix: Budget for at least one substantial amendment. Better yet, invest in thorough protocol design upfront — including feasibility assessments and investigator input — to reduce amendment likelihood.
Red flag #3: Technology costs buried in ‘overhead’
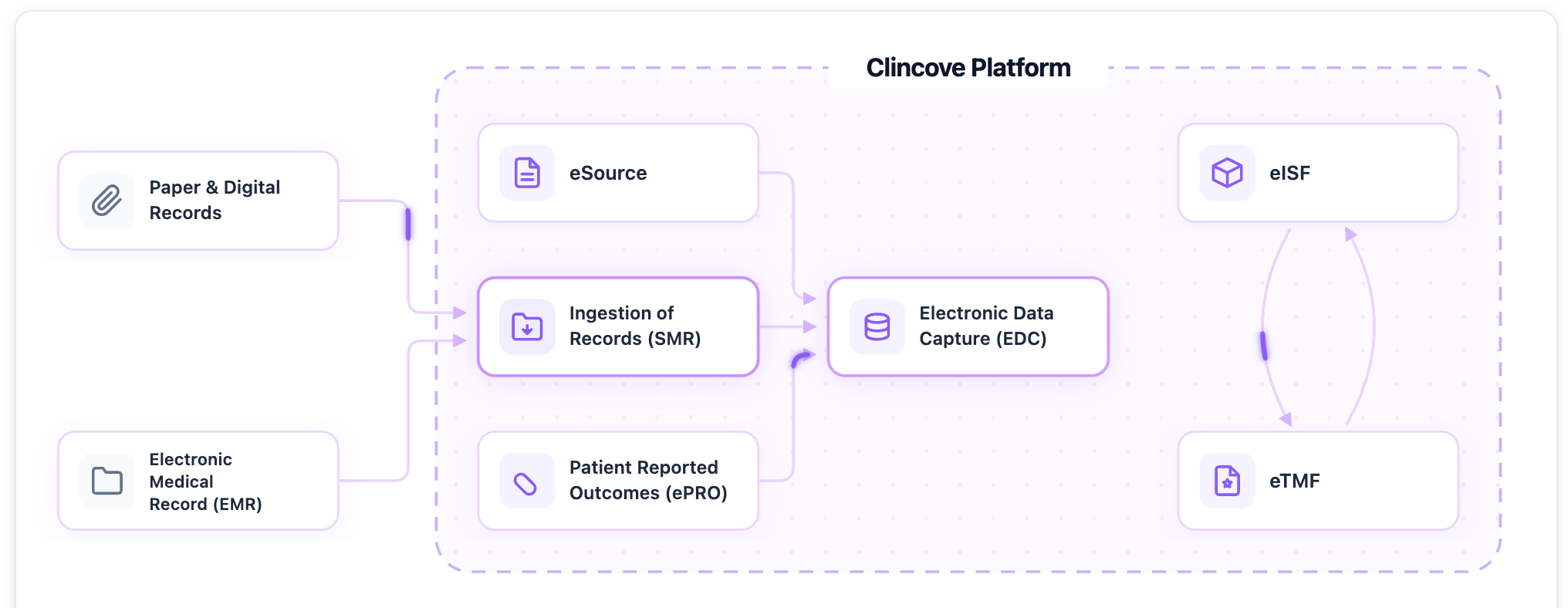
When EDC, eTMF, RTSM, and safety database costs are lumped into a single ‘technology’ or ‘overhead’ line item, it’s impossible to evaluate whether you’re overspending. Five separate platform licenses add up fast.
Fix: Itemize every technology platform. Then ask whether a unified platform could replace multiple point solutions at lower total cost. The savings from eliminating data silos alone often justify the switch.
Red flag #4: Monitoring budget based on calendar, not risk
If your monitoring budget assumes monthly on-site visits to every site regardless of performance, you’re spending money where it isn’t needed and possibly underspending where it is.
Fix: Adopt risk-based monitoring. Allocate on-site visit budget based on site risk profiles and KRI signals. Read our complete RBM guide.
Red flag #5: No contingency for timeline extensions
Extended timelines are expensive: ongoing site fees, CRO costs, safety monitoring, and opportunity cost. If your budget has zero contingency for a 3–6 month extension, one enrollment delay will blow it up.
Fix: Include 10–15% contingency for timeline extensions. Fund strategies that reduce this risk: better site selection, realistic enrollment targets, and technology that accelerates site activation.
For a comprehensive approach to trial budgeting, read our Complete 2026 Budget Planning Guide. Or see how Clincove reduces total trial costs through platform consolidation.
Continue Reading

Clinical Trial Operations Planning: The 2026 Checklist Every Sponsor Should Download (Clinical Trials Planning Template Included)
Improve study planning with a free clinical trial operations template covering budgets, milestones, vendors, risks, comp

Decentralized Trials in 2026: What’s Working and What Isn’t
DCTs promised to revolutionize clinical research. Three years post-pandemic, we look at what’s actually delivering resul
Protocol AI: How We Built CRF (Case Report Forms) Auto-Generation - Modernizing EDC
A behind-the-scenes look at how Clincove’s Protocol AI reads protocol documents and automatically generates case report
Simplify clinical operations
Ready to modernize your clinical trials?
See how Clincove unifies EDC, eISF, eTMF, and eSource into one platform -- deploy in weeks, not months.